Dental fluorosis has a very typical presentation in terms of tooth surface appearance and oral distribution. Overall, there is increasing clinical evidence for reducing the severity of fluorosis during adolescence for all permanent teeth and into early adulthood. The teenagers in Riyadh participated in this cross-sectional study. 383 kids were included through practical sampling after Riyadh's schools were contacted. Fluorosis was found to be 26% prevalent overall, according to the findings. The most frequent form of fluorosis was described as "very mild," and the least frequent form was described as "questionable." Fluorosis in the teeth is less common than it once was. The age of participants had no significant impact on the prevalence or severity of dental fluorosisAccording to Dean's index of fluorosis, 1% of people had uncertain dental fluorosis, 42% had very mild fluorosis, 25% had mild fluorosis, 17% had moderate fluorosis, and 15% had severe dental fluorosis (Figure 3). Additionally, age groups were used to compare the prevalence of dental fluorosis, but there was no statistically significant difference (p-value:.725). The overall prevalence of dental fluorosis is on the lower side. Prevalence as well as severity of dental fluorosis was not significantly associated with the age of participants.
Introduction
Dental fluorosis is a disease that affects the teeth and is caused by long-term increased exposure to fluoride during tooth development [1, 2]. Ingestion of fluoride from drinking water during tooth development up to age six can contribute to the development of fluorosis. It is clinically characterized by hypo mineralization tooth cloudiness and brown discoloration (staining) surface. Although fluoride is considered effective in preventing tooth decay, excessive fluoride intake can put bones and teeth at risk of developing dental fluorosis [3]. The degree of dental fluorosis can range from very mild to severe, depending on the number of affected flanks (proportion of teeth) and the extent of physical damage to the teeth [4].
This fluoride-containing enamel increases porosity and exposes the surface to other conditions such as tooth decay, extrinsic staining sensitivity, and malocclusion. The person is exposed to excess fluoride and individual differences or susceptibilities. Dental fluorosis as a condition to be treated inevitably informs public interest in local health and government. Therefore, understanding the severity and importance of risk factors associated with this disease and monitoring and controlling improvement measures [5, 6].
When it comes to the way that dental fluorosis manifests in the mouth and on the surface of teeth, it is extremely common. The crystals seem regular, but when the intercrystalline gaps get wider, pores form. Along with increasing fluorosis severity, the concentration of fluoride in the enamel as well as its porosity, content, and depth of involvement all rose. The post-secretory or early maturation stage is the most crucial time for the onset of fluorosis, according to clinical studies of tooth fluorescence [7].
In Madhya Pradesh, India, many young people suffer from dental fluorosis. In Madhya Pradesh, early adolescent dental fluorosis was present 40.5% of the time. The amount of fluoride in the water is positively connected with the degree of dental fluorosis. The best indicator of dental fluorosis was the water's fluoride concentration [8].
Overall, there is increasing clinical evidence for reducing the severity of fluorosis during adolescence for all permanent teeth and into early adulthood. Researchers should consider declining dental levels when studying fluorosis in adolescents, and policymakers should consider this trend when making appointment fluoride intake recommendations [9].
Fluoridation has helped to reduce caries prevalence for the past 70 years by encouraging remineralization and preventing demineralization in the mouth [10]. In at least 25 countries, fluorosis is believed to be a widespread problem. The Syrian and Turkish fluoride belts, as well as Iraq, Iran, Afghanistan, and India-to-Northern Thailand-to-China fluoride belts, have been identified. It's possible to find both of these fluoride belts in the area. The belts of the Americas and Japan are very similar. Risk factors for dental fluorosis include beverages, foods, and toothpaste. Adults and adolescents with a high caries risk should use a dentifrice with 5000 ppm fluoride [11].
Fluorosis was examined in the schools of the UK which compared the children with teenagers and showed that fluorosis in teenagers was more which is 25% at 15 years old. The dental examination revealed incisor damage, tooth surface loss (TSL), and enamel opacity (age 12 only). Stains on teeth that couldn't be removed by brushing were sent to parents and children in a questionnaire [12].
Fluoride poisoning can be caused by drinking groundwater with a fluoride level of more than 1.5 mg/L. 370 children from Zhijin, Guizhou, China, were discovered to have fluorosis. Children between the ages of 12 and 16 were more likely to develop dental as well as skeletal fluorosis [13].
Fluoride contamination of Pakistan's groundwater is widespread. There is a wide range of fluoride concentrations in groundwater. Increased fluoride absorption can cause tooth discoloration in children whose teeth are still forming and high prevalence supports that fact [14].
Study rationale
The findings of this study will help in planning an educational program for parents and children to create awareness regarding dental fluorosis.
Study hypotheses
Dental fluorosis is high among the teenagers of Riyadh City.
Aims of the study
Materials and Methods
Study design
This is a cross-sectional study conducted among the teenagers of Riyadh.
Study sample
Schools in Riyadh were contacted and 383 students were included using convenient sampling.
Sample size calculation:
Confidence level: 95%
Population Size: 100000
Margin of Error: 5%
Sample size: 383
Study instrument
Data was recorded on a paper with the age of the teenager mentioned. An oral examination was conducted using wooden tongue depressors. All teeth of 383 teenagers were examined and Dean’s index of fluorosis was used to record the findings.
Dean’s Index of Fluorosis:
0=Normal
1=Questionable
2=Very mild
3=Mild
4=Moderate
5=Severe
Statistical analysis
With the help of SPSS version 22, both descriptive and inferential statistics were carried out on the collected data. The significance level was kept under 0.05 when comparing the groups. With a significance level kept under 0.05, a chi-square test was used to compare the results based on age groups.
Reliability
IRB approval
This proposal was registered to the REU research center web portal and the IRB was received as well.
Results and Discussion
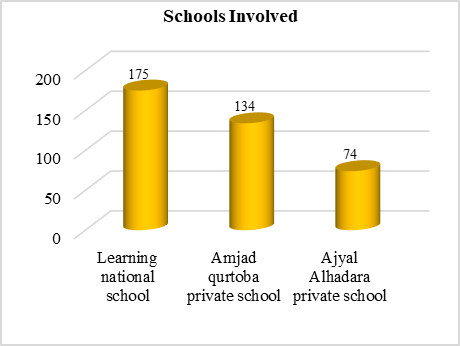
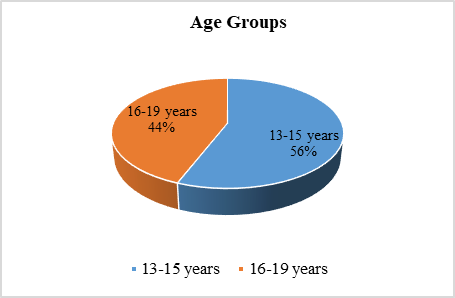
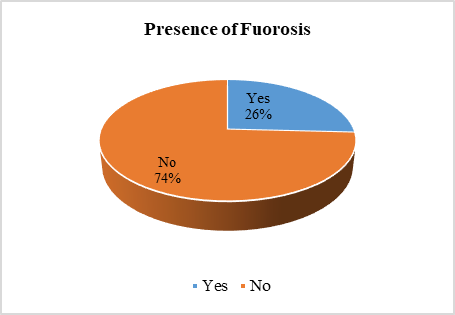
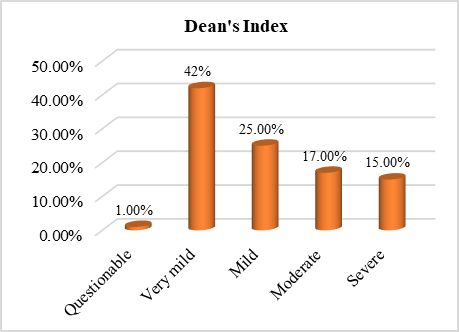
Three schools—Learning National School (175 students), Amjad Qurtoba Private School (143 students), and Ajyal Alhadara Private School (74 students)—contributed a total of 383 teenage students who took part in the study (Figure 1). Based on age (13–15 years and 16–19 years), the subjects were split into two groups. In terms of the percentage of each group, 44% of those between the ages of 16 and 19 and 56% of those between 13 and 15 years old were included (Figure 2). The primary goal of the study was to determine the prevalence of dental fluorosis, and it was found that 26% of people had it (Figure 3). According to Dean's index of fluorosis, 1% of people had uncertain dental fluorosis, 42% had very mild fluorosis, 25% had mild fluorosis, 17% had moderate fluorosis, and 15% had severe dental fluorosis (Figure 4). Additionally, age groups were used to compare the prevalence of dental fluorosis, but there was no statistically significant difference (p-value = 0.725). The Dean's measure of fluorosis prevalence was also evaluated, but no statistically significant difference (p-value = 0.759) was found (Table 1).
|
|
|
Figure 1. Number of participants involved from each school |
|
|
|
Figure 2. Age groups of study participants |
|
|
|
Figure 3. Prevalence of dental fluorosis among all participants |
|
|
|
Figure 4. Prevalence of various types of fluorosis |
|
Table 1. Prevalence of dental fluorosis among the study participants |
|||
|
|
13-15 years |
16-19 years |
P-value |
|
Prevalence of dental fluorosis |
Present: 26.6% Absent: 73.4% |
Present: 24.8% Absent: 75.2% |
0.725 |
|
Prevalence according to Dean’s Index of Fluorosis |
Questionable: 0% Very mild: 38% Mild: 28% Moderate: 17% Severe: 17% |
Questionable: 2% Very mild: 47% Mild: 23% Moderate: 16% Severe: 12% |
0.759 |
The goal of this study was to figure out how common dental fluorosis was among teenage boys living in Riyadh City. Findings showed that 26% of people had fluorosis as a whole. While the least common form of fluorosis was described as "questionable," the most common form was "very mild." A similar study done by Okoye et al. among teenagers in Nigeria exhibited that the prevalence of dental fluorosis was 11.3%, which is considerably low compared to our study [15]. They also compared their findings based on gender, which did not apply to our study as all participants were boys.
Another study conducted in Dammam by Khan et al. revealed a dental fluorosis prevalence of 33% among teenagers, which included a much higher proportion of ‘questionable’ and ‘moderate’ types of fluorosis as compared to our study [16]. They also compared their findings based on gender, which did not apply to our study as all participants were boys. According to Verma et al.'s investigation in Karnataka, India, 64.3% of adolescents were found to have dental fluorosis among 1026 registered students, and more than 50% of them were found to have severe or moderate fluorosis based on the Dean's Fluorosis Index [17]. These figures far exceed what our research revealed.
To determine the prevalence and severity of dental fluorosis, a study was carried out among schoolchildren in several British cities. According to the data, the entire population's prevalence of fluorosis was 36.5%. The authors also divided their subjects according to their intake of fluoridated water [18]. However, this comparison of fluoridated vs. non-fluoridated water was not included in our study. Another study by Avocefohoun et al. in Benin found that 115 of the 560 schoolchildren who were tested had severe fluorosis, translating to a prevalence of 20.53% [19]. As a consequence of their research, a correlation between this fluorosis and age, body surface, and either housing or water sources serving schools has been found. These outcomes are higher than what was observed in our study, as severe fluorosis was found to be in only 15% of the teenagers. However, our study did not show any statistically significant association between age and prevalence.
In a separate study done in northern India, it was discovered that 4.1% of kids there had dental fluorosis. While nearly 86% of the samples had healthy tooth enamel, only 9.3% of the students displayed potentially dangerous fluorosis symptoms. Additionally, fluorosis in its very mild and mild forms was discovered in 1.3 and 1.8% of samples, respectively. Around 1% of samples had moderate fluorosis enamel surfaces that were clearly worn and frequently disfigured by brown staining [20]. These results were far less than what we saw in the study results.
Limitations of the study
Conclusion
Acknowledgments: We would like to acknowledge the support of the REU research center.
Conflict of interest: None.
Financial support: None.
Ethics statement: This study fulfills the ethical requirement of the REU ethical committee.