Zirconia is generally utilized as a framework for the rest of all-ceramic crowns, typically needing feldspar ceramic veneering to achieve suitable esthetics as it offers high opacity. Monolithic zirconia restorations have been presented lately, and their manufacturing process needs attention. This systematic review aimed to determine the difference between monolithic and layered zirconia crowns regarding their clinical success and longevity. A thorough analysis of the literature covering the years 2012–2023 was done, using the ScienceDirect, Medline, and PubMed databases. The terms that were employed were "monolithic zirconia", "layered zirconia", "longevity", and "aesthetics". The procedure for choosing the articles that were searched was outlined using the PRISMA flowchart. From 112, we recruited 10 studies after a comprehensive screening process. Most of the included studies suggested that the clinical success rate and fracture resistance were superior among monolithic zirconia crowns compared to the multilayered ones. However, some studies revealed no significant difference between the two. Therefore, further studies are required to provide more evidence of whether monolithic zirconia possesses higher longevity and clinical success.
Introduction
Nowadays, a vast range of restorative materials is offered to fabricate indirect restorations. Nevertheless, dental zirconia is considered to be the most wanted one due to its adaptability, conjoining high strength with adequate esthetics, permitting an utterly digitized manufacturing process, and allowing supplementary individualization via orthodox ceramic layering techniques [1-5].
Clinically based evidence plays a vital role in differentiating the survival and durability of one material in competition with the other. It is commonly known that metal-based restorations are dependable and long-lasting options for indirect restorative techniques. Reports state that after 11 years, 95% of metal-ceramic restorations were still intact and functioning well. On the other hand, the cost of noble metal alloys has significantly increased recently. Moreover, owing to their wear resistance, biocompatibility, shade stability, low heat conductivity, and aesthetics, metal-free ceramic indirect restorations are in higher demand. Nowadays, ceramic restorations are often used in dental operations [6-10].
Several all-ceramic restorative materials have been presented during current times, out of which yttria-stabilized polycrystalline tetragonal zirconia became popular in dentistry for its satisfactory mechanical properties and biocompatibility. Zirconia is generally utilized as a framework for the rest of all-ceramic crowns, typically needing feldspar ceramic veneering to achieve suitable esthetics as it offers high opacity. Monolithic zirconia restorations have been presented lately, and their manufacturing process needs attention [10-15].
Previous literature has revealed that the utmost mean marginal gap value was documented for monolithic zirconia. However, layered zirconia crowns revealed the lowermost mean marginal gap values. It was also concluded by several studies that monolithic zirconia restorations had a better marginal adaptation as compared to layered zirconia restorations. Nonetheless, both restorations have a satisfactory, marginal fit [15-19].
PICO question
Is there a difference in the clinical success and longevity (Outcome) of monolithic (Comparison) and layered zirconia (Intervention) crowns among patients (Population) requiring these restorations?
Aims of the study
The purpose of this systematic review was to determine the difference between monolithic and layered zirconia crowns when it comes to their clinical success and longevity.
Materials and Methods
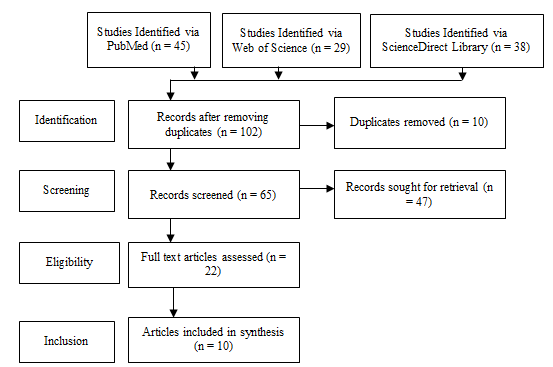
Using the ScienceDirect, Medline, and PubMed databases, a comprehensive review of the literature published between 2012 and 2023 was conducted. "Monolithic zirconia," "layered zirconia," "aesthetics," and "longevity" were the phrases used. The PRISMA flowchart was used to explain the process for selecting the articles that were searched (Figure 1).
Inclusion criteria
Exclusion criteria
|
|
|
Figure 1. PRISMA Flow Diagram |
Risk of bias assessment
As indicated in Table 1, the studies' quality was assessed using the Cochrane risk of bias assessment approach.
|
Table 1. Summary of Cochrane Risk of Bias Assessment |
|||||||
|
Study |
Selection Bias/Appropriate control selection/baseline characteristics similarity |
Selection bias in randomization |
Selection bias in allocation concealment |
Performance-related bias in blinding |
Reporting bias/Selective reporting of outcomes |
Detection bias Blinding outcome assessors |
Accounting for confounding bias |
|
De Paula et al. (2019) |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
|
Choi et al. (2020) |
+ |
- |
+ |
+ |
+ |
+ |
+ |
|
Alraheam et al. (2023) |
+ |
+ |
- |
+ |
+ |
+ |
+ |
|
Waldecker et al. (2022) |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
|
Altamimi et al. (2014) |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
|
Malament et al. (2019) |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
|
Mohammed et al. (2019) |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
|
Kasem et al. (2023) |
+ |
+ |
+ |
+ |
+ |
- |
+ |
|
Pihlaja et al. (2016) |
+ |
+ |
+ |
+ |
+ |
+ |
+ |
|
Mahmoud et al. (2020) |
+ |
+ |
+ |
- |
+ |
+ |
+ |
Results and Discussion
Monolithic and layered zirconia are found to be very popular dental restorations nowadays. This study is designed to investigate the success rate of both crowns in clinical performance in terms of efficacy and longevity.
According to de Paula et al. [20], When compared to bi-layered crowns with even thickness (Bi-EV) at 20% and 4% and bi-layered crowns with modified core design (Bi-M) at 17% and 2%, the monolithic crown (MON) demonstrated a much greater level of dependability. Only the monolithic crown group showed a 7% crown survival rate after three million cycles. Bi-M (573,384) had the lowest average longevity, MON (1.73E + 06) had the highest, and Bi-EV (619,774) had the intermediate lifespan. Most people agree that MON crowns are the most trustworthy. The fatigue durability of these crowns is unaffected by the modified framework design (Table 2).
Choi et al. [21] showed that after hydrothermally aging translucent monolithic zirconia ceramics, higher phase transitions and surface microstructure alterations were seen. Surface roughness and oxygen concentrations increased, but zirconium and yttrium concentrations dropped. Multilayered zirconia ceramics became more opaque, while conventional zirconia ceramics became more translucent. Mechanical characteristics were reduced with increasing aging time, and different forms of fabrication influenced the properties of these ceramics.
Abd Alraheam et al. [22] showed that the Resin-bonded zirconia (Adh-Zr) performed better than glass ionomer cemented zirconia (GIC-Zr) and resin-bonded lithium disilicate (Adh-LD) in marginal adaptation, except for other quality outcome measures where there were no statistically prominent differences between the groups. Regarding anatomic shape, marginal adaptation, and color match, layered zirconia crowns perform considerably better than monolithic ones. Both adhesively bonded and conventionally cemented zirconia are acceptable treatment choices with excellent short-term efficacy rates. More extensive follow-up clinical investigations are required to examine their long-term efficacy rates.
Weldecker et al. [23] revealed that the 5-year success rate for Monolithic Zirconia Single Crown (MZ-SC) was 95.8%, while the 5-year rate for Partially Veneered Zirconia Single Crown (PZ-SC) was 87.0%. Clinical application of MZ-SC and PZ-SC can be accomplished with excellent medium-term survival and success rates, as well as unaffected esthetic outcomes (Table 3).
Altamimi et al. [24] compared fracture resistance of bi-layered zirconia fluorapatite in standard coping (Group A) and anatomical coping (Group B) with monolithic lithium disilicate (Group C). In Group C, catastrophic fractures occur, while veneered fractures were found in Groups B and A. Group C demonstrates more fracture resistance than others. In Groups A and B, ceramic fracture resistance is more in B than in A.
Malament et al. [25] demonstrated that the cumulative survival percentage after ten years was 99.6%. At 10.4 and 7.9 years, the cumulative survival rate for 550 bi-layered e.max complete-coverage restorations and 1410 monolithic restorations was 100% and 96.5%, respectively. A total of 3380 years were in danger due to seven failures of monolithic complete-coverage restoration units. There were no failures in bi-layered complete-coverage restorations, with a total time at risk of 1733 years. According to the study, pressed lithium disilicate restorations had an overall failure rate of less than 0.2% annually and performed well over ten years.
Mohammed et al. [26] showed that zirconia frameworks are veneered utilizing the CAD-on approach with IPS e.max CAD blocks, and zirconia-based restorations exhibit greater marginal and internal adaptability. The accuracy of zirconia-based restorations is compromised when veneering zirconia frameworks with glass-based ceramics using a hand layering technique. This affects both internal and marginal accuracy. Internal and marginal adaptation of restorations based on zirconia have a positive correlation. Veneered zirconia-based and monolithic CAD/CAM restorations are typically linked to poor occlusal adaptation.
Kasem et al. [27] revealed that according to the Kaplan–Meier survival method, the overall survival rate was 100% of both zirconia-reinforced lithium silicate and monolithic high translucency zirconia. During the 36-month follow-up, it was noted that in comparison to the face location, the mesial and distal sites had higher increases in periodontal probing depth. Between the two materials, there was, however, no statistically significant difference seen. Both could be utilized as a repair material for teeth that have been vertically prepared. After three years of clinical research, both ceramic materials produced good aesthetic outcomes and supported stable, healthy soft tissues without mechanical difficulties.
Pihlaja et al. [28] conducted a study to assess the success and survival rates of layered Nobel-Procera Zirconia, Zirkonzahn Zirconia, and monolithic Prettau Zirconia for fixed dental prostheses (FDPs) using Kaplan-Meier survival analysis. Out of the 76 persons who were tested, 75 percent of them had received 88 zirconia FDPs. The duration of the follow-up period was 4.9 years, with a range of 3 to 7 years. The most prevalent issue observed in 14.7% of the 88 FDPs was the chipping of the veneering porcelain. After 4.9 years, both zirconia-based partial FDPs had a 100% survival rate.
Finally, Mahmoud et al. [29] investigated the wear and chipping characteristics of both layered and monolithic zirconia. There was no chipping, and every restoration was reported as alpha. For the wear test, there was no substantial difference between both restorations. After a year of clinical use, both showed good mechanical features with no chipping. For both materials, clinically acceptable wear of the opposing enamel was observed (Table 3).
|
Table 2. Analysis of the included studies (Meta-analysis) |
|||
|
Study |
monolithic |
layered zirconia |
P-value |
|
De Paula et al. (2019) [20] |
1.12 (0.83–1.51) |
1.02 (0.78–1.35) |
<0.005 |
|
Choi et al. (2020) [21] |
3.91 ± 0.18 |
5.54 ± 0.33 |
<0.005 |
|
Alraheam et al. (2023) [22] |
3.98 ± 0.15 |
3.91 ± 0.29 |
<0.005 |
|
Waldecker et al. (2022) [23] |
N/A |
N/A |
- |
|
Altamimi et al. (2014) [24] |
1.360 |
1.014 |
<0.005 |
|
Malament et al. (2019) [25] |
2.396 |
2.279 |
>0.005 |
|
Mohammed et al. (2019) [26] |
80.55 |
82.46 |
>0.005 |
|
Kasem et al. (2023) [27] |
18.00 |
20.00 |
<0.005 |
|
Pihlaja et al. (2016) [28] |
N/A |
N/A |
- |
|
Mahmoud et al. (2020) [29] |
1.066 |
1.052 |
>0.005 |
|
Meta-analysis results |
14.04 |
14.65 |
>0.005 |
|
Table 3. An overview of the traits and conclusions of the 10 research that were included. |
||||||||
|
Authors |
Study design |
Sample size |
Restoration no. |
Restoration type |
Follow-up (years) |
Manufacturing technique |
Clinical performance |
Conclusive findings |
|
De Paula et al. (2019) |
Randomized control trial |
30 |
3 |
Bi-layered crowns with even-thickness (Bi-EV), Monolithic crowns (MON), and Bi-layered crowns with modified core design (Bi-M) |
3 |
Lost wax casting technique |
Survival rate = 47-19% , 20-4% and17-2% at 1-2 million cycle Mean life = 1.73E + 06, 619,774, and 573,384 for MON, Bi-EV and Bi-M, respectively |
Monolithic lithium disilicate crowns with a modified framework design outperformed bi-layered crowns in terms of mean life and survival probability when loaded at marginal ridges. |
|
Choi et al. (2020) |
Randomized control trial |
60 |
270 |
Translucent monolithic zirconia conventional and multilayered |
3-4 |
Milling and grinding machine and hydrothermal aging |
All of the materials' mechanical, optical, and surface characteristics were impacted by hydrothermal aging. |
Transparent monolithic zirconia's surface characteristics vary with age; conventional materials get more transparent while multilayered materials become more opaque, changing the materials' qualities. |
|
Alraheam et al. (2023) |
Retrospective study |
35 |
218 |
resin-bonded zirconia (Adh-Zr), Glass ionomer cemented zirconia (GIC-Zr), and resin-bonded lithium disilicate (Adh-LD) |
1.85 |
Cementation |
Compared to monolithic zirconia, Layered zirconia has much greater quality outcomes regarding anatomic shape, marginal adaptation, and color match. |
Zirconia and LD crowns offer high short-term success rates, with selective cutting back and layering improving aesthetics without compromising integrity. Clinical trials requiring greater sample numbers and longer follow-up periods are necessary for long-term success. |
|
Waldecker et al. (2022) |
Randomized control trial |
68 |
162 (90 MZ-SC and 72 PZ-SC) |
Monolithic (MZ-SC) and veneered zirconia single crowns (PZ-SC) |
5 |
Cementation |
Survival rate = 87%, 95.8% (complication-free) 93.1%, 96.2% (failure-free) 100%, 98.6% (ceramic-fracture free) for MZ-SC and PZ-SC respectively |
Only biological problems cause failures in MZ-SC and PZ-SC, which have a high medium-term survival without compromising esthetic qualities. |
|
Altamimi et al. (2014) |
Randomized control trial |
30 |
30 |
Bi-layered zirconia standard coping (A), anatomical coping (B), and monolithic lithium disilicate (C) crowns |
- |
Lost wax method |
Fracture strength = 561.87 N for A, 1014.16 N for B, and 1360.63 N for C |
C presented more fraction resistance than A and B. Between A and B, B showed increased ceramic fracture resistance. |
|
Malament et al. (2019) |
Randomized control trial |
556 |
1960 |
Monolithic, Bi-layered complete-coverage and lithium disilicate, restoration. |
10.4 |
glass-ceramic pressing system and Lost-wax method |
The survival rates for lithium disilicate, monolithic, and bi-layered complete-coverage restorations are 99.6%, 96.5%, and 100%, respectively. |
Over ten years, lithium disilicate restorations, which were mostly limited to molar teeth, had a modest failure rate of 0.2% annually. |
|
Mohammed et al. (2019) |
Randomized control trial |
40 |
3 |
Monolithic zirconia crowns, veneered zirconia frameworks (Manual, press-on, CAD-on layering technique) |
- |
Milling machine |
Pearson's correlation test found a significantly positive correlation (r=0.1305) between marginal and internal fit. |
Veneering zirconia CAD-on frameworks show superior marginal and internal adaptation than zirconia-based restoration. |
|
Kasem et al. (2023) |
Randomized control trial |
40 |
2 |
zirconia-reinforced lithium silicate and monolithic high translucency zirconia |
3 |
constructed using CAD/CAM technology and sealed with a dual-polymerizing luting resin |
100 % survival rate |
Premolar regions are suitable for minimally invasive vertical restorations using monolithic high translucency zirconia and zirconia-reinforced lithium silicate ceramics with a margin thickness of 0.5 mm. |
|
Pihlaja et al. (2016) |
Retrospective study |
76 |
88 |
Layered Zirkonzahn Zirconia and layered Nobel- Procera Zirconia and Monolithic Prettau Zirconia |
3-7 (mean 4.9) |
Zirkonzahn Zirconia, Prettau Zirconia by Manual milling, and Nobel- Procera Zirconia by computer-aided design/ computer-aided manufacture (CAD/CAM) |
100 % survival rate 89 % success rate |
Zirconia is suitable for pre-doctoral dental education for partial FDPs, with chipping porcelain veneering problematic but repairable without compromising restoration aesthetics. |
|
Mahmoud et al. (2020) |
Randomized control trial |
34 |
2 |
Veneered zirconia crowns and Monolithic zirconia single crowns |
1 |
CAD/CAM software |
100 % survival rate |
The clinical study found that after a year of usage, an exceptionally transparent monolithic veneer, Katana, with full coverage polish demonstrated good mechanical qualities and less enamel wear than monolithic zirconia. |
The primary goal of monolithic or multilayer restorations is to reunite form, function, and esthetics while causing minor damage and extending the life of the remaining natural dentition. Today's cutting-edge technology in these fields can produce above-average to outstanding aesthetic outcomes. The clinical decision between the two can be influenced by several criteria, of which clinical efficacy and longevity are most important [29-35].
The current study addressed the longevity of anatomically important monolithic and bilayer lithium disilicate crowns with and without core design changes. Changing the underlying architecture of bilayer crowns did not significantly increase their survival or mean life. To compare the previous research, some laboratory and clinical studies show that monolithic ceramic crowns used at the manufacturer's suggested thickness outperform veneered crowns. After the porcelain veneer with its poor fracture toughness is removed, the fatigue performance of the monolithic bulk material is determined by its fracture toughness, processing processes, and thickness. 70% of the crystal volume of lithium disilicate is integrated into a glass matrix to create a glass ceramic with thin, elongated grains 1.5 and 0.4 meters in diameter [36-44].
Konstantinidis et al. examined 65 posterior crowns for a year. Short-term survival rates were relatively high, with 98.5% success and 100% survival. This was due to discoloration at one crown's margin [12]. One study looked at 101 people who had 148 posterior monolithic zirconia crowns, with an average length of 25.0 years. The results showed that, even after 3.5 years, 91.5% of these crowns were still in use. Throughout the observation time, six concerns surfaced. Five of the fractures were biological, while one was technological. Longitudinal fractures, hypersensitivity, pulpitis, and use as an abutment for a novel prosthetic treatment technique were among the biological fractures [45-55].
This retrospective study examines the success rate of lithium disilicate and zirconia crowns that are partly laminated and adhesively and cementally attached in faculty practice settings. The study discovered that patients' compliance with every crown significantly reduced the risk of subsequent caries. However, the study results are limited by the short follow-up period. The short sample size can limit statistical significance. The study's shortcomings include its retrospective design and brief follow-up period, which are uncommon in the dental literature. Future studies should examine the long-term efficacy of partly fitting and monolithic crowns. Similar to the Adh-Zr and Adh-LD crowns, the GIC-Zr crown had a success rate. The success rate of monolithic crowns was similar to that of partly stacked crowns [55-64].
The objective of this study was to provide current data on the rates of complications, survival, and success of ceramic restorations for a brief duration of three years. Over a medium time frame, the study gathered longitudinal data on the aesthetic results and clinical efficacy of monolithic and partly veneered zirconia single crowns. When the study was compared to a prior three-year study, it was discovered that biological issues and crown removal brought about by a different treatment strategy were the only reasons for additional difficulties with monolithic crowns. In crowns with partial veneers, no more issues arose. The study center's functional approach limited the use of veneers to the esthetic zone, resulting in an imbalanced distribution of monolithic and partially veneered crowns between the front and back sections. Most problems happened in monolithic crowns, which decreased the chance of MZ-SC patients surviving without difficulties. Previous clinical investigations have indicated a higher frequency of problems for posterior crowns, which suggests that the position of the crowns played a role in this. The low prevalence of anterior issues and the uneven distribution of monolithic and partly veneered crowns in the front and posterior areas are the study's shortcomings [26, 64-73].
The findings reveal a noteworthy distinction between the two bi-layered groups and the monolithic lithium disilicate group, which may have resulted from the fluorapatite glass-ceramic material's lesser strength when contrasted with lithium disilicate. Zirconia cores did not fracture, while fluorapatite veneer was the leading cause of fractures in bi-layered groups. An abutment is essential to increase the monolithic crown's strength, but additional evidence is required to consider the crown's overall thickness and adhesion factor. However, the abutment support was repeatable because using a metal die, the substrate for cement adherence was not comparable to natural tooth structures' mechanical characteristics. Since the cement used in the trial was ordinary and not chemically active, adhesion, which would have benefited the glass ceramic group, was not a significant concern [8, 73-82].
In contrast to earlier research, the data show that the effect of confounding factors on the durability of lithium disilicate was very minor in this study. There was variation among the participants in terms of age and gender, which might have an impact on the results. To identify the characteristics influencing the long-term robustness of lithium disilicate restorations and associated materials, this study also looked at 25 other variables. From a clinical standpoint, it is worth mentioning that there was a high likelihood of 99.1% and 98.2% for sex determination and 99.6% for tooth position correctness. Furthermore, the likelihood of failure for restorations using alternate ceramic materials was much greater. Out of the 7 failures, 5 occurred on molar teeth, with 4 of them specifically affecting second molars. Molars pose a challenge for ceramic restorations due to their high occlusal load-bearing capacity [61, 82-91].
As a result of the material contraction that occurs during sintering, pre-sintered zirconia restorations acquire a denser and more durable crown. The crown dimensions must be increased using the CAD/CAM system to account for this size reduction. Several studies have examined the correlation between crown dimensions and fit. According to them, larger crowns result in more significant sintering contraction and, consequently, less crown adaptation [91-94].
Ibrahim et al. [95] assessed the breakage of veneered and monolithic zirconia in full-coverage posterior dental restorations. Based on the data, there was no significant difference in enamel wear between veneered and monolithic zirconia. However, there was also no significant difference in enamel wear specifically for monolithic zirconia. The polished appearance of both restorations could be the cause of this. All crowns were reported as alpha, and chipping studies revealed no distinction in chipping behavior between veneered and monolithic zirconia [95, 96].
Conclusion
Both monolithic as well as multilayered zirconia crowns are beneficial and successful when it comes to rehabilitation. Most of the included studies suggested that the clinical success rate and fracture resistance were superior among monolithic zirconia crowns compared to the multilayered ones. However, some studies revealed no significant difference between the two. Therefore, further studies are required to provide more evidence of whether monolithic zirconia possesses higher longevity and clinical success.
Acknowledgments: None.
Conflict of interest: None.
Financial support: None.
Ethics statement: This study received ethical approval from Riyadh Elm University (FUGRP/2023/329/1031/926).