The evolution of esthetic restorative materials for anterior teeth has transformed the field of dentistry, driven by the demand for natural-looking and durable dental restorations. This narrative review explores recent advancements in anterior teeth esthetics, focusing on materials, techniques, and technologies. Through a systematic literature search of academic databases, studies published in the last decade were analyzed to highlight innovations in materials such as ceramics, zirconia, resin-based composites, and digital technologies like CAD/CAM and 3D printing. The review also examines the benefits and limitations of various esthetic restorative materials and crowns, emphasizing the importance of selecting appropriate materials and techniques for optimal esthetic outcomes. The development of new esthetic crowns, including open-faced SSCs, preveneered SSCs, strip crowns, resin-retained crown forms, and Pedo Pearls, offers various solutions tailored to different clinical scenarios. Despite these advancements, challenges such as technique sensitivity, cost, and the need for continued research remain. Future directions should focus on further improving the durability, esthetic quality, and ease of application of restorative materials to enhance patient satisfaction and clinical outcomes.
Introduction
Facial and dental esthetics are crucial in prosthetic and prosthodontic treatments. Four key components of esthetic dental treatments include (a) contour, (b) color, (c) Functional Parameters (d) arrangement, the size, shape, and visibility of teeth, and gingival esthetics are vital for restoring patients' esthetics [1, 2]. Facial aesthetics is also greatly influenced by the midline of the teeth and the face. Prosthetic teeth with the right proportions blend in harmoniously with the rest of the face. The goal of aesthetic restorative therapy for anterior teeth should be to get the best possible aesthetic result. Additionally, facial features are crucial when choosing teeth for patients undergoing prosthetic rehabilitation [3, 4].
The anterior teeth play the most crucial role in smile aesthetics, with symmetry of the anterior teeth, including hard and soft tissues, being a key factor. Considering these aspects, an ideal treatment plan must focus on improving this symmetry to provide patients with the most aesthetically pleasing restorations [5, 6].
Literature search strategy
A systematic literature search was performed using multiple academic databases to conduct a comprehensive narrative review of recent advancements in anterior teeth aesthetics. The search was primarily carried out in PubMed, Scopus, Web of Science, and Google Scholar. The following keywords and phrases were used:
Boolean operators such as "AND," "OR," and "NOT" were utilized to refine the search and ensure a thorough examination of the topic.
Inclusion and exclusion criteria
Inclusion criteria
Exclusion criteria
Data extraction and analysis
Once the relevant articles were identified, the following data were extracted and analyzed:
Quality assessment
The quality of the selected studies was assessed using the following criteria:
Synthesis of results
The data extracted from the selected studies were synthesized to provide a comprehensive overview of the recent advancements in anterior teeth aesthetics. The synthesis involved:
Limitations of the review
This narrative review acknowledges the following limitations:
Results and Discussion
Biomaterials for esthetic restorations
The selection of biomaterials for esthetic restorations in anterior teeth requires careful consideration of their shade and clarity. Human teeth exhibit a variety of shades, from opaque to translucent areas, necessitating a balance between these properties to achieve an optimal esthetic outcome [6, 7].
Ceramic/Zirconia
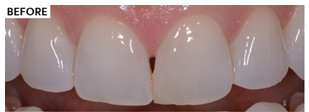
Anterior porcelain veneer restorations play a crucial role in restoring the shape and color of teeth while also creating contact between adjacent teeth, thereby enhancing the horizontal stability of the dental arch and improving patient aesthetics (Figure 1). Porcelain veneers and crowns effectively address teeth discolorations caused by trauma, fluorosis, and tetracycline exposure [8-10]. These restorations are fabricated using computer-aided design and computer-aided manufacturing (CAD/CAM) methods. Advances in these technologies now allow for the fabrication of these restorations in a single day through faster sintering processes that yield excellent esthetic and mechanical properties [11, 12].
|
|
|
(a) |
|
|
|
(b) |
|
Figure 1. Ceramic anterior restorations |
Resin-based composite (RBC)
Commercially available RBCs are highly esthetic due to their opaque and translucent materials. Opaque shades are typically used for inner restorations or for defining margins, while translucent shades are applied as final layers or for incisal translucencies. These are often labeled as "dentin" for opaque shades and "enamel" for translucent shades [13-16].
Despite their benefits, RBCs have limitations, such as lower fracture resistance and surface instability compared to ceramic restorations. However, these issues have been mitigated with the development of newer composites like micro-hybrid composites, nano-filled, and nano-hybrid composites. Improvements in RBCs over recent decades include enhanced optical properties and biocompatibility. The development of these materials has enabled clinicians to replicate the shade and translucency of natural teeth more accurately. Different layering techniques are recommended to achieve superior esthetic results. Furthermore, composite restoration failures, such as shade adjustments or shape modifications, can be easily repaired, whether immediately or on older restorations [10, 17-19].
Esthetic materials
Composite resin restorative materials, ionomer-modified resins or compomers, resin-modified glass ionomers, and conventional glass ionomers are among the aesthetic materials available for anterior restorations. Because composite resin materials are so strong, resilient to wear, aesthetically pleasing, and capable of matching colour, they are frequently the material of choice for repairing anterior teeth. However, they are technique-sensitive and require the use of acid etching and bonding agents, making them intolerant of moisture and hemorrhage (Figure 2).
Compomers share many characteristics with composite resins, including similar esthetics and handling, but offer some fluoride release and slightly better moisture tolerance. Although they are less aesthetically pleasing and have lower wear resistance than composite resins, resin-modified glass ionomers emit fluoride, don't need to be etched, and are less susceptible to moisture [20-22].
|
|
|
(a) |
|
|
|
(b) |
|
Figure 2. Anterior composite rehabilitation |
Nanomaterials
High mechanical resistance to wear and fracture, minimal polymerization shrinkage, superior polishing, colour stability, and outstanding optical qualities including transparency and fluorescence are all provided by nano-composites (Figure 3). These properties make them suitable for anterior and posterior restorations. The nano-composite Filtek Z350 XT, composed of silica nanoparticles and silane-coated zirconia, provides excellent physical and mechanical properties due to the incorporation of small-sized filler particles into the resin matrix [9, 23].
|
|
|
(a) |
|
|
|
(b) |
|
Figure 3. Nano-composite anterior restorations |
Top of FormBottom of FormDigital waxing
Recent advancements in digital dentistry have introduced digital waxing as a promising alternative to conventional waxing techniques. Digital waxing is the process of virtually changing dental morphology by a variety of techniques, including mirror imaging of an undamaged neighboring tooth, fitting an average tooth, and employing a biogeneric library. Digital waxing presents several clear benefits over traditional techniques, such as less material handling and fewer processes that are prone to error. As a result, the total execution time and cumulative errors are reduced.
One of the significant benefits of digital waxing is the integration of software that allows the quantification of treatment effects before the active phase. This capability enables precise critiques of dental treatments, focusing on esthetic outcomes, material thickness, and the potential invasiveness of preparation. The use of digital technologies thus ensures more predictable and controlled results, which is particularly beneficial for enhancing anterior teeth aesthetics [24-26].
Despite the numerous advantages, the fastest workflow, identified as the 3D digital workflow, received the worst ratings in a survey. This discrepancy could be attributed to the limitations of open-source software used in the study. These limitations include the inability to place dental arches in occlusion and the lack of digital dental elements for the digital wax-up process. In contrast, the 2D digital workflow, although time-consuming with an operative time of 400 minutes, provided accurate dental and facial analyses, leading to more customized previsualization and aesthetic results that align well with the patient's facial features. With adequate training, operators might reduce the time required for these procedures (Figures 4 and 5).
Cost differences among the various workflows are a critical consideration for clinicians. The feasibility of using open-source software was tested to make digital tools accessible to young and non-specialized clinicians. The 2D digital workflow facilitated symmetrical reconstruction in terms of tooth size and gingival arch shape, offering great aesthetic outcomes and effective patient communication. However, the 3D workflow requires further evaluation to optimize its application and improve its ratings [27-29].
|
|
|
(a) |
|
|
|
(b) |
|
|
|
(c) |
|
|
|
(d) |
|
Figure 4. Digital waxing of anterior teeth |
|
|
|
(a) |
|
|
|
(b) |
|
|
|
(c) |
|
|
|
(d) |
|
|
|
(e) |
|
Figure 5. Digital waxing of anterior teeth |
|
Table 1. Benefits and limitations of esthetic dental materials |
||
|
Material |
Benefits |
Limitations |
|
|
|
|
|
Ceramic/Zirconia |
- High esthetic quality and natural appearance |
- Can be brittle and prone to fracture |
|
- Excellent color stability and translucency |
- Higher cost compared to other materials |
|
|
- Strong and durable with good mechanical properties |
- Requires significant tooth preparation |
|
|
- Digital technologies (CAD/CAM, 3D printing) enhance precision and efficiency |
- Technique-sensitive during fabrication and placement |
|
|
Resin-Based Composite (RBC) |
- Highly esthetic with good color matching and translucency |
- Lower fracture resistance compared to ceramics |
|
- Can be easily repaired or modified |
- Surface instability and wear over time |
|
|
- Versatile layering techniques for superior esthetic results |
- Technique-sensitive and requires moisture control |
|
|
- Newer composites (micro-hybrid, nano-filled, nano-hybrid) have improved properties |
||
|
Composite Resin Materials |
- Superior strength, wear resistance, and esthetics |
- Technique-sensitive, requiring acid etching and bonding agents |
|
- Excellent color-matching capabilities |
- Intolerant of moisture and hemorrhage |
|
|
Compomers |
- Good esthetics and handling similar to composite resins |
- Slightly inferior physical properties compared to composite resins |
|
- Fluoride release |
||
|
- Better moisture tolerance than composite resins |
||
|
Resin-Modified Glass Ionomers |
- Fluoride release |
- Inferior esthetics and wear resistance compared to composite resins |
|
- Less sensitive to moisture |
||
|
- Does not require etching |
||
|
Glass Ionomer Cements (GICs) |
- Self-curing and chemically bonds to tooth structure |
- Inferior physical properties and esthetics compared to other materials |
|
- Fluoride release |
- Primarily used in situations with economic constraints or minimally invasive procedures |
|
|
- Moisture tolerant |
||
|
Nano Materials |
- High mechanical resistance to fracture and wear |
- Requires specialized handling and knowledge |
|
- Low polymerization shrinkage |
- Maybe costlier due to advanced technology |
|
|
- Excellent polishing and color stability |
||
|
- Good optical properties (fluorescence and translucency) |
||
|
- Suitable for both anterior and posterior restorations |
||
|
Digital Waxing |
- Reduces material manipulation and error-prone steps |
- 3D digital workflow may have limitations in occlusion placement and lack digital dental elements |
|
- Decreases execution time and accumulated inaccuracies |
- 2D digital workflow is time-consuming despite the accuracy |
|
|
- Allows for precise critiques of dental treatments before the active phase |
- Cost differences among workflows can be significant |
|
|
- Enhances esthetic outcomes through digital previsualization |
- Open-source software may limit the effectiveness of some workflows |
|
Esthetic crowns
Open-Faced stainless steel crowns (SSCs)
A substantial amount of cavities in the anterior teeth can be restored with stability and durability using open-faced SSCs. Even with very little tooth structure left, these crowns are easily fitted and crimped on all surfaces and are fracture-resistant. However, the primary drawback of SSCs is their unique silver color. The open-face SSC technique addresses this issue by removing the metal on the facial surface of the crown and replacing it with tooth-colored resin. This chairside procedure, although time-consuming and requiring meticulous hemorrhage control, significantly improves the esthetic appearance [29].
Despite the challenges, SSCs are sometimes preferred for anterior teeth, particularly mandibular incisors, where esthetics is less critical. SSCs have a reported retention rate of 93% after 27 months, indicating their long-term reliability. The open-face technique is cost-effective and enhances the appearance compared to the original metal color, making it a viable option for aesthetic restoration in certain clinical scenarios [30].
Preveneered stainless steel crowns
Preveneered SSCs were introduced to offer an esthetic alternative for anterior restorations in pediatric dentistry. These crowns feature a prefabricated tooth-colored material bonded to the facial surface of SSCs, typically using resin-based composite material. This design allows for placement in areas with poor hemorrhage control, providing an improved white appearance (Table 1).
Various brands, including Nusmile Signature Crowns, Cheng Crowns, Kinder Crowns, and Flex White Faced Crowns, offer these pre-veneered options. However, challenges such as wear on the incisal edge and potential fractures of the facial portion are common. Repairing chipped sections is difficult, often necessitating the replacement of the entire crown if the metal becomes exposed. Additionally, crimping the facial portion can easily fracture the esthetic facing; thus, retention relies on crimping the lingual portion [31].
The application of these crowns requires careful handling to avoid fracturing the prefabricated resin portion. Glass ionomer cement is recommended for securing the crown in place until it sets. Preveneered SSCs have a retention rate exceeding 90% after 6 to 17 months, demonstrating their effectiveness as an esthetic solution for anterior teeth despite the noted limitations.
Strip crowns
Strip crowns, composed of celluloid crown forms, are utilized as matrices filled with tooth-colored materials, predominantly resin-based composites. These composites are chosen for their ability to match the shade of adjacent teeth, providing excellent esthetic outcomes. In younger children, resin-modified glass ionomer cement is often employed as an interim restoration material. The placement of strip crowns is a technique-sensitive procedure that necessitates stringent moisture and hemorrhage control to prevent contamination of the resin with blood or saliva. Adequate remaining tooth structure is essential to ensure proper bonding [32].
Once the resin-based composite is polymerized, the celluloid form is removed easily with a dental bur or sharp blade. Special considerations are necessary when placing strip crowns over pulpectomy-treated teeth filled with iodoform paste. To avoid the yellow hue of the paste showing through the crown, either opaque resin should be used, or the iodoform paste should be removed below the cervical area. Similarly, when zinc-oxide eugenol is used after pulpal treatment, it is recommended to place a glass ionomer or resin-modified glass ionomer base over it to ensure proper polymerization during light exposure. These protocols are critical in maintaining the esthetic integrity and functional longevity of strip crowns.
Resin-Retained crown forms
In addition to strip crowns, two primary alternatives exist for resin-retained crown forms that bond to the tooth structure. The first alternative is a crown made of tooth-colored plastic. This crown is filled with resin material and fitted to the tooth after etching and bonding. Notably, there is no need to remove the crown form after polymerization. However, reshaping the crown with a bur is not feasible as the plastic material may deform from the heat.
The second alternative involves a crown made from resin composite material, which can be reshaped with a finishing bur to achieve a more aesthetically pleasing appearance. Care must be taken to reduce the tooth adequately before placement; otherwise, forcing the crown onto the tooth can cause it to crack or fracture. These resin-retained crown forms offer versatile options for achieving desirable aesthetic results while accommodating various clinical situations [33].
Pedo pearls: Metal crown forms
The Pedo Pearls are a new kind of crown that is presently being developed and tested in the field. They are made of metal and resemble stainless steel crowns, but they are painted with tooth-colored epoxy. Since the epoxy coating sticks to aluminum better than stainless steel, aluminium is used to make these crowns. In permanent dentition, aluminium crown forms are already often employed as temporary crowns. However, their relative softness makes them difficult to maintain over time, particularly in places with high occlusion where the white coating could flake off.
Pedo Pearls may provide reasonable aesthetics and the simplest implantation procedure of all the crown varieties. Different luting cements are used to cement stainless steel crowns to teeth. Cement containing zinc phosphate and polycarboxylate have historically been utilized. Still, adhesive cements such as glass ionomers and resin-modified glass ionomers are now preferred for their superior retention and reduced microleakage. Reduced microleakage can decrease the incidence of clinical failures due to recurrent caries, pulpal pathology, and coronal microleakage. Therefore, the use of adhesive luting cements, particularly glass ionomer, is recommended for better clinical outcomes [34].
Intra-coronal restorations
Primary teeth can be restored intracoronally using a variety of materials, such as resin composites, glass ionomer cement, resin-modified ionomers, and resins modified with polyacid. Every material has unique benefits and drawbacks, and the clinical circumstances at the time of installation have a big impact on the selection of material. For a variety of reasons, full coronal restoration of primary incisors is frequently required. The crowns used for these restorations include directly bonded resin crowns and luted stainless steel crowns (Table 2).
Despite the availability of these options, no single type of crown has been conclusively proven superior under all clinical circumstances because of the absence of supporting data. Additionally, restorative materials for mandibular incisors remain limited, even though caries in the mandibular region are not common, neither stainless steel crowns nor celluloid crown forms are made especially for this area (Table 2). This gap highlights the need for continued research and innovation in materials and techniques to improve restorative solutions for all primary teeth [34-36].
|
Table 2. Benefits and limitations of esthetic crowns |
||
|
Material |
Benefits |
Limitations |
|
Open-Faced Stainless Steel Crowns (SSCs) |
- Durable and stable for extensive caries |
- Unesthetic silver color without modification |
|
- Resistant to fracture |
- Time-consuming and technique-sensitive during facial resin application |
|
|
- Easily fitted and crimped with minimal remaining tooth structure |
||
|
- Cost-effective |
||
|
- High retention rate (93% after 27 months) |
||
|
Preveneered Stainless Steel Crowns |
- Improved esthetic appearance with tooth-colored facial surface |
- Wear on the incisal edge and potential fractures of the facial portion |
|
control |
sections, often requiring full crown replacement |
|
|
- Various brands available (Nusmile, Cheng, Kinder, Flex White) |
- Crimping the facial portion can easily fracture the esthetic facing |
|
|
- High retention rate (over 90% after 6-17 months) |
||
|
Strip Crowns |
- Excellent esthetic outcomes matching adjacent teeth |
- Technique-sensitive with stringent moisture and hemorrhage control required |
|
- Interim restoration material option for young children |
- Adequate remaining tooth structure essential for bonding |
|
|
- Easily removed celluloid form after polymerization |
- Special considerations needed for pulpectomy-treated teeth with iodoform paste |
|
|
Resin-Retained Crown Forms |
- Two alternatives: tooth-colored plastic and resin composite |
- Tooth-colored plastic crown cannot be reshaped with a bur due to heat deformation |
|
- Tooth-colored plastic crown requires no removal after polymerization |
- Resin composite crown can crack if the tooth is not adequately reduced |
|
|
- Resin composite crown can be reshaped for superior esthetics |
||
|
Pedo Pearls: Metal Crown Forms |
- Potentially easiest placement technique among crowns |
- Soft aluminum material poses long-term durability challenges |
|
- Provides reasonable esthetics |
- White coating may wear off in heavy occlusion areas |
|
|
- Improved adhesion with epoxy coating on aluminum |
||
|
- Adhesive luting cements (glass ionomer) reduce microleakage and clinical failures |
||
|
Intracoronal Restorations |
- Various materials (resin composites, glass ionomer cement, resin-modified ionomers, polyacid-modified resins) available based on clinical conditions |
- No single material has proven superior under all circumstances |
|
- Full coronal restorations are necessary for various reasons |
- Limited restorative solutions for mandibular incisors |
|
|
- Options include directly bonded resin crowns and luted stainless steel crowns |
- Continued research and innovation needed to improve solutions for primary teeth restorations |
|
Conclusion
Recent advancements in anterior teeth esthetics have significantly enhanced the capabilities of dental professionals to achieve superior esthetic results. Innovations in materials such as ceramics, zirconia, and resin-based composites have improved both the mechanical properties and the visual appeal of restorations. Digital technologies like CAD/CAM and 3D printing have revolutionized the fabrication process, allowing for more precise and efficient production of esthetic restorations. The development of new esthetic crowns, including open-faced SSCs, pre-veneered SSCs, strip crowns, resin-retained crown forms, and Pedo Pearls, offers various solutions tailored to different clinical scenarios. Despite these advancements, challenges such as technique sensitivity, cost, and the need for continued research remain. Future directions should focus on further improving the durability, esthetic quality, and ease of application of restorative materials to enhance patient satisfaction and clinical outcomes.
Acknowledgments: None.
Conflict of interest: None.
Financial support: None.
Ethics statement: None.